
Image of a brain, courtesy of the Epilepsy Foundation
Seizure Diaries: My Seizure Life
A wave of electrical shocks passed over the man, through his body and around his brain, as he fell to the ground on a busy street. His pulsating and spastic shaking were violent and erratic. Some people turned away, probably thinking: “Why was he doing that? Is he on drugs? Was he trying to freak people out? He must be faking it, right?” Other people recognized the signs of seizure and shouted for help. A family doctor in the crowd, didn’t know what to do, so he called 9-1-1 and asked for an ambulance. Finally, the seizing man’s wife arrived, she had received an electronic notification of his seizure. She knelt down and reassuringly whispering in his ear, “I am here.”
Once revived and feeling better, the man acknowledged, “I know my seizures scare people, even doctors seem scared to death watching someone in a seizure. I have no control over when a seizure occurs or how severe it will be.” The man says he has learned that there are many reasons how and why they occur. That man is Charlie Hooper.
His life as a person saddled with seizures continues.
Reasons for Seizures
Some of the reasons seizures occur are because of:
- Stress
- Flashing Lights
- Heat
- Missing Medication
- Nicotine
- Loud Sounds
- Over-Exerting One’s Self
- Lack of Sleep
- Anxiety
- Headaches
- Structural Brain Abnormalities
- Congenital Malformations
- Strokes
- Tumors
- Cysts
- Acquired Brain Injures
Primary Generalized Epilepsy
Petit mal, also known as “absence seizures,” and grand mal seizures are forms of primary generalized epilepsy. A list of the generalized versions are listed on the graphic below. These seizures are not caused by a metabolic derangement, although doctors say that “such a derangement can lower that person’s seizure threshold and provoke seizures in a person with generalized epilepsy whose seizures were previously controlled by medication.”

Even people without epilepsy can suffer from a seizure which looks just like grand mal epilepsy. The massive grand mal seizures can be caused by various metabolic conditions ranging from low blood sugar (hypoglycemic) and low sodium (hyponatremia), to certain medications or abrupt withdrawal of alcohol, or substances upon which the brain has become dependent. Metabolically induced seizures are different from Epilepsy because they don’t automatically imply that some people will be subject to the recurring seizures unprovoked by a metabolic disturbance that caused them in the first place. Once these metabolic conditions are corrected the patient should not be at risk for recurrent seizures, whereas the epileptic patient, like Charlie, is.

Charlie’s Seizure Life
In his own words, Charlie talks about how it used to be: “When I was about to have a seizure, I appeared to be distracted. People said I was rude, because I focused on something else. My stare and attention were not on them or our conversation. That distracted pause was often how it started. Before I knew what hit me, I became completely disoriented and the seizure took over!”
Today, Charlie’s seizures are various “partial” and “focal” types, of differing intensity and duration. Some seizures originate in a large variety of places, called “foci,” in his brain and can spread like wild-fire to adjacent regions. And these seizures can go on to become “generalized tonic-clonic episodes.” These are the most common type of epilepsy and it is often related to structural abnormalities within the brain, like congenital malformations, strokes, tumors and other problems.
The word tonic means stiffening and clonic means rhythmic jerking. The tonic phase comes first with muscles stiffening, a cry or groan, and the person losing consciousness and falling to the floor. The clonic phase is when the person’s arms and legs begin to jerk rapidly and rhythmically at the joints (elbows, knees, and hips) and the person’s breathing can cause foaming at the mouth. Sometimes the person loses bladder or bowel control as their body relaxes and the seizure subsides.
In 2016 Charlie received his Neuropace implant. Since then his seizures have decreased substantially from an average of 94 a month to about 51 a month. At the same time the seizures have become less severe. He tells his caregivers, “I used to getting 15 seizures a day. They were mainly Gran Mals (or Tonic Clonic Seizures) and now are mostly Complex Partial and Focal Seizures. These days I am down to fewer than 5 seizures a day. And they are less debilitating.”
Charlie’s Focal Seizures last for different lengths of time. He has tried to analyze how he experiences them. Charlie writes about one Focal Seizure: he calls it a ten second focal, where: “I sometimes feel I can actually talk myself out of it, but I still experience minor symptoms.” And he writes about a twenty second focal seizure, which is impossible to handle, because of its acuity and duration.

The Start of Seizures
When Charlie was in his twenties, his father took him to a neurologist at Johns Hopkins because of some night time episodes that appeared to be seizures. The neurologists discovered a few unique aspects of Charlie’s brain from an MRI and a CT scan: One was that he had a series of large congenital arachnoid cysts located on the frontal lobe of the left hemisphere. Secondly, the doctors located a partial agenesis of the corpus callosum on his right hemisphere. These two congenital abnormalities, especially the large number and size of the cysts, had wrecked havoc on his homunculus, which lies between his motor and sensory cortexes. These abnormalities made for some atypical electrical transfers in Charlie’s brain from one hemisphere to the other.
One physician remarked, “I can honestly say, I have never seen multiple arachnoid cysts as big as Charlie’s.” And Charlie’s neurologist from Johns Hopkins conferred with a neurosurgeon, when the surgeon spotted the cysts in the first CT scan, he thought that Charlie needed immediate life-saving surgery. Charlie never had that surgery. The doctors and their staff concluded that it was best to leave well enough alone, given that these were congenital cysts. They did not want to risk disrupting the equilibrium Charlie had achieved, living with them all of his life.
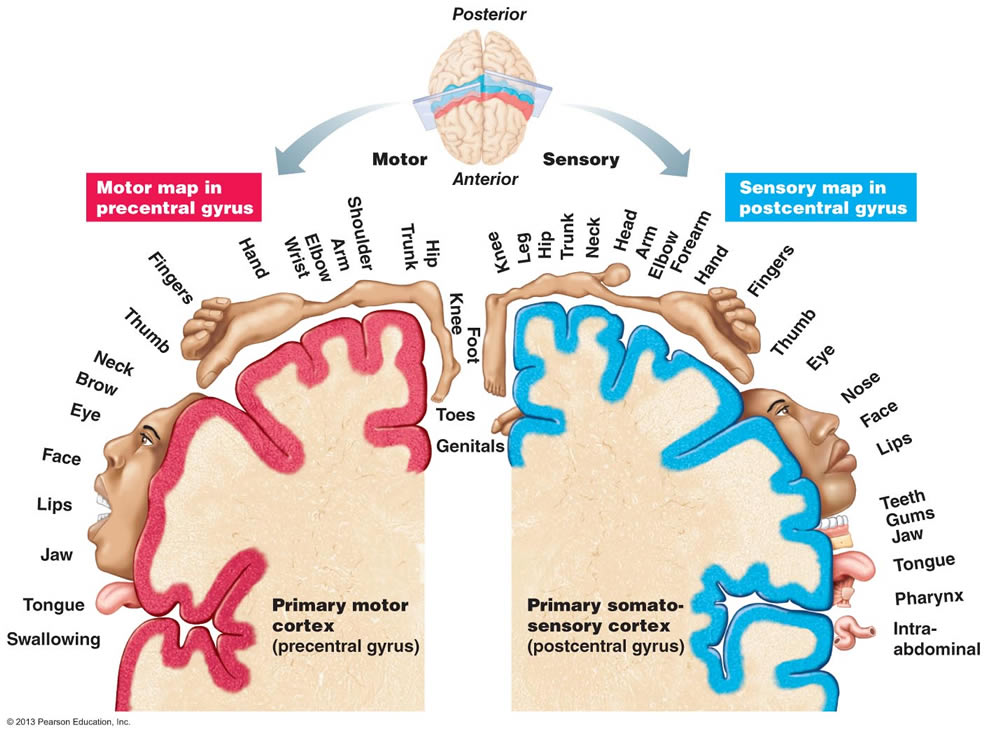
The Sensory and Motor Homunculus Lies Between the Hemispheres
Thirteen+ years ago, the seizures became so violent and frequent that they forced Charlie to stop working. With the help of his sister, Nancy, he was able to qualify for Social Security Disability Benefits (SSDI). Since that time, Charlie’s wife, Steph, has had to handle the brunt of the family’s financial responsibilities.
Charlie cannot drive, work, ride a bike, or walk in the park, without a caregiver or support person. He knows how little SSDI payments provide his family, and he realizes that his brain disorder has destroyed many of his dreams: “One of my career goals was to become a Police Officer. I had served for years in the field as a security guard and I was on my way to gain a good police position, until the Epilepsy took over. I know that I would be an officer today, if it were not for Epilepsy.”
Focal Epilepsy
Dr. Millie LaFontaine is a retired neurologist. She is also Charlie’s sister. Dr. LaFontaine offered a perspective on Charlie’s risks with seizures. “I agreed with the Hopkins doctors when they decided to leave the cysts alone. Removing them would not likely improve his seizures (and could well make them worse). In general, surgery carries a high risk of creating more problems than it solves.”
Dr. LaFontaine went on to describe in greater detail the seizure type that Charlie is living with: “Focal epilepsy, which is what I believe Charlie has, is actually much more common than metabolic seizures. Focal epilepsy can result from the host of insults to the brain that any of us may become unfortunate enough to be born with or to acquire, such as traumatic brain injury, strokes, tumors, infections or blood clots. The thing that is so different in Charlie’s case is his multiple foci, which results in an astounding variety of seizures, and has been appallingly refractory to treatment. That his dignity shines through, despite what he’s dealing with, is all the more indication of the strength of his character!”
Before the Neuropace implant operation, the Tonic Clonic Seizures were acute. Charlie says, “I would be in intense pain for up to 15 minutes and, most of the time, I would just pass out. I could be out cold for anywhere from 45 minutes to a couple of hours.” Dr. LaFontaine compares Charlie’s seizures to lightning strikes: “For some seizures, Charlie went into them with a fire extinguisher, but there were so many foci, the lightning strikes were everywhere and they all started fires.” The conflagration caused Charlie’s whole body to fall victim to the violent episodes.
Charlie’s wife, Steph, has timed many of his seizures for his diaries. Steph says that now Charlie has more of the five-minute Tonic Clonic Seizures and fewer of the longer episodes. And Charlie experiences fewer of those five minute seizures every month since the operation. The month before the operation, those debilitating Tonic Clonics were the majority of his seizures.
Charlie has also talked with a neurologist, who specializes in headaches. A keen observer of his patterns, Charlie often noticed that when he was having a Migraine headache, that pain was a precursor of an oncoming epileptic episode. “I saw those headaches as a sign of a seizure in the making. I did not know exactly when, but it was about to occur. In my diary I noticed that I used to get headaches AFTER a seizure, and now I was noticing them BEFORE the episode.” The neurologist has noticed the same patterns and has prescribed medication to help arrest the pain.

Many of Charlie’s family members have experienced Migraine headaches, including his mother. Dr. LaFontaine says that some neurologists have prescribed anti-convulsant medications for their Migraine and Epilepsy patients, hoping that they can stop both conditions; however, no sure-fire “migra-leptcy” medicines out there seem to be without severe side-effects.
Charlie’s Conviction: Tell the Story
Over the years, Charlie continues to notice the stigma and ignorance of his family, friends and neighbors around Epilepsy. As he tells his story, Charlie emphasizes that it is not something you catch, like the flu. It is not infectious and it is not contagious. Yet people are so nervous when the word Epilepsy enters into the conversation, they shut down. They go on to report how scary it is to witness any seizure victim, much less one with chronic Epilepsy.
Charlie realizes that his life with Epilepsy is his personal journey. First caused by his congenital brain malformation, he has had to adapt his life to the new realities.
As he says, “The doctors have told me that my seizures were dormant for the first 22 years of my life. It took a highly stressful event, the death of my mother, to start the first seizure. I have had seizures going on 32 years now. In that time, I have taken almost every seizure medicine that the market has to offer. And I have had two surgeries to place medical devices in my body. The first one in 2006, was called ‘Vagus Nerve Stimulator.’ The VNS implant is attached to the Vagus Nerve. Its main objective is to stop the petit mal seizures. It did not have any effect on my grand mal seizures. Then, ten years later in 2016, I had a new type of implant. Called ‘Neuropace,’ it is a device placed inside my brain to slow down and hopefully stop my seizures. I was the 852nd person to ever receive this implant.”

Neuropace implant device
The Neuropace surgery was done at the Penn State Hershey Medical Hospital. For a majority of the recipients, after the adjustment period, their seizures stopped within six months. Due to Charlie’s brain malformations, even though the Neuropace was implanted 18 months ago, he is still in the adjustment period. He says with a smile, “I am known as a ‘Unique Case.’ That’s for sure. With my cysts and my focal epileptic seizures, I am one of a kind.”

The manufacturer of the Neuropace implant, sends someone to attend each of Charlie’s neurology appointments. They are there to help with the electrical adjustments needed. The neurologist, since they are at a teaching hospital, also have med students who come into the room for appointments. “It can get crowed with all of these soon-to-be doctors who want to observe.” Neuropace has given Charlie a laptop. He uses it daily to scan his head to detect seizure activity. These scans help the doctors make micro-adjustments to the brain implant. When he has neurological appointments, he now gets to see the seizure activity from the doctors’ powerful computer.

Despite it all, Gratitude
One of the hardest parts of his life with Epilepsy is for Charlie to see Steph taking on the roles as the family’s primary caregiver and sole financial bread winner.
Charlie Hooper is a man of gratitude: “Steph is a true champion in my heart! She accepts the caregiving role and she loves me. Steph is always there as my personal protector! She is the most honest person and the sweetest woman I have ever known! I feel so blessed to have her in my life. No one realizes how much she has sacrificed for me, and I truly love her for her selflessness and dedication.”
